The Impact of Running on Brain Function and Mental Health
Post by Megan McCullough
The takeaway
A 10-minute running session of moderate intensity was shown to increase mood and executive function through the bilateral activation of the prefrontal cortex
What's the science?
Previous research has shown that physical exercise can lead to an increase in mood and executive function through the activation of the dorsolateral prefrontal cortex. These studies have predominantly measured the effects of exercise on the brain by using pedaling as the form of exercise. Since running uses different muscles and parts of the body, it may have different effects on the brain than other forms of exercise. This week in Scientific Reports, Damrongthai and colleagues studied the effects of running on mood, executive function, and the prefrontal cortex.
How did they do it?
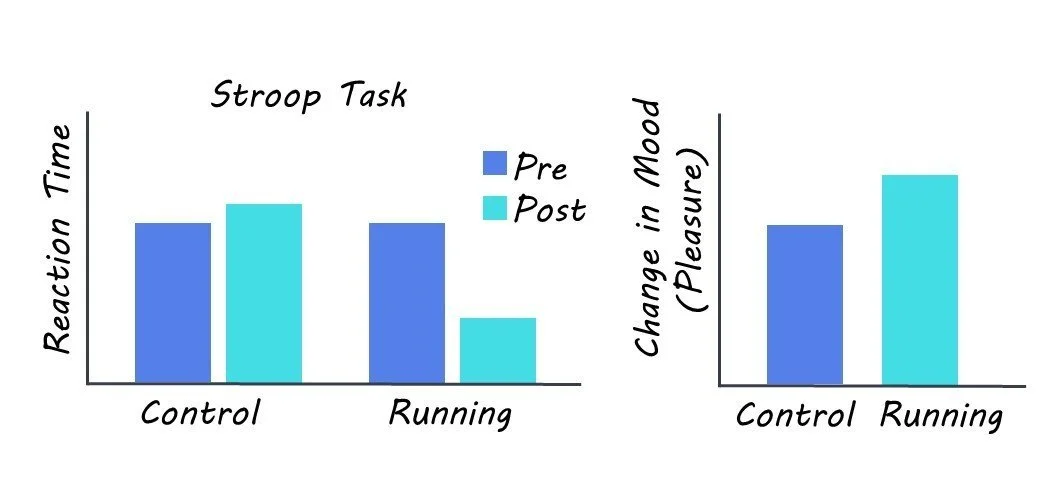
The participants consisted of 26 healthy individuals that completed both a 10 minute run at moderate intensity and a control resting period in a randomized order. After both activities were completed, executive function was then evaluated using the colour-word matching Stroop task. This task involves a list of names of colours, written in different colours; participants are tasked with naming the colour the word is written in and not the word itself. The Stroop test was used to test executive function because it measures the ability of participants to control their responses despite external lures. Mood was also measured before and after exercise using a mood scale the states of arousal and pleasure the participant was in. Finally, functional near-infrared spectroscopy was used to measure blood flow and thus activation in the prefrontal cortex.
What did they find?
The authors found higher blood flow in the prefrontal cortex after running trials compared to after the resting control trials. This suggests that running increased bilateral activation in the prefrontal cortex, an area associated with cognition and mood. The authors also found that participants performed better at the Stroop test after the moderate exercise compared to control trials. This shows the positive effect of running on cognition. Finally, the authors found that running led to an increase in mood, in particular an increase in pleasure level that has never been found in their previous pedaling studies. Together, these results suggest that a moderately intense running session can lead to improvements in cognition and mood through bilateral activation of the prefrontal cortex.
What's the impact?
This study adds to the growing body of research showing that physical activity benefits mental health. Critically, this research shows that running — a whole-body locomotion exercise — is also an effective way to achieve improvements in mood, especially pleasure level, which can benefit exercise adherence and executive function.